
An internationally agreed-upon set of definitions and criteria for vitiligo have been developed. Find out what they are!
International experts hope the development of new international consensus statement defining severity and relapse for vitiligo will close a much-needed gap.
Vitiligo is the most common depigmentation disorder in the world but there is no agreed upon definition for what constitutes a relapse of the condition. The assessment of vitiligo severity is also highly reliant on the perspective of the treating clinician.
The lack of consistent terminology in these spaces is becoming a problem for clinicians who manage chronic dermatological conditions
“In the dawn of a new therapeutic era for several emerging treatments for vitiligo, the lack of definitions for the terms severity and relapse became apparent when assessment reports were produced for regulatory authorities and funding bodies for reimbursement purposes,” the authors of a new consensus statement for the severity and relapse for vitiligo wrote in JAMA Dermatology.
“To address this gap, we conducted an international, multidisciplinary consensus study to define vitiligo severity and relapse using methods that incorporated perspectives from both experts and people with lived experience across diverse regions, skin phototypes and ethnic backgrounds.”
The large-scale project involved a literature review to establish a foundational framework for the development of the consensus statement, interviews and focus groups with people living with vitiligo to explore their thoughts and experiences of severity and relapse, an international Delphi study and a final consensus meeting to approve the relevant definitions and criteria.
Relying solely on the body surface area (BSA) of pigment loss as a measure of disease burden was deemed to be insufficient. Instead, the group proposed a new assessment model:
- Mild vitiligo: vitiligo affecting less than three percent of a patient’s BSA.
- Moderate vitiligo: vitiligo affecting 3-10% of BSA.
- Severe vitiligo: vitiligo affecting ≥10% BSA OR vitiligo that is rapidly progressing/spreading, regardless of the level of BSA involvement.
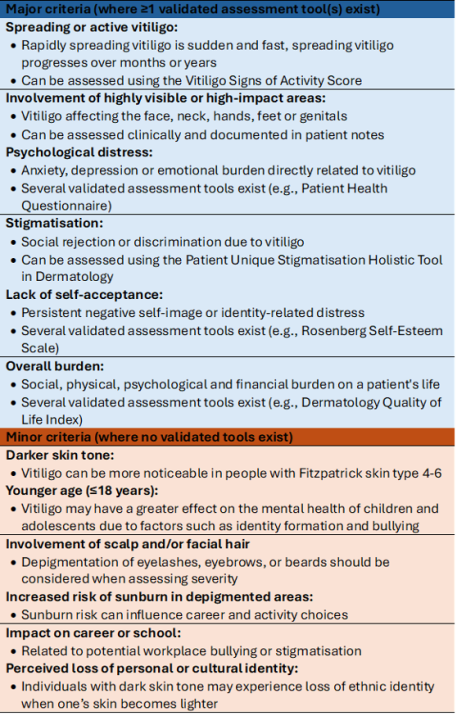
Moderate cases could be upgraded to severe if one or more major clinical and psychosocial criteria are present, or if two or more minor criteria are present:
“There are important practical considerations when applying severity criteria, especially in the context of significant variations in health care policies, access to treatments and cultural factors,” the authors wrote.
“Severity is not a static measure; it necessitates frequent review and adaptation in response to changing circumstances.
“Aspects of severity associated with effects on cultural, social and psychological life such as stigma, marriage prospects and employment should be considered during clinical consultations and recorded accordingly in clinical notes as evidence.
Related



“Although several validated instruments were discussed, severity grading should not rely solely on questionnaire scores. Instead, it should combine clinical judgment with shared decision-making to reflect each patient’s lived experience.
“[And] for rapidly spreading (rapidly progressive) vitiligo, which was defined as the existence of a large number of new depigmented spots or significant enlargement of existing depigmented spots over the past three months, consensus was reached that irrespective of the percentage of BSA involved, patient should be classified automatically into the severe category.”
The consensus statement recommended that systemic therapy would be appropriate in patients with moderate to severe vitiligo, as well as in patients with rapidly progressive vitiligo. However, the group noted that systemic therapy should only be used if at least 12 weeks of topical therapy has failed to garner a response.
“[But] systemic therapy should be warranted based on multiple factors and treatment failure with a topical therapy should not be the sole reason to institute systemic therapy,” the authors of the consensus statement noted.
A relapse of vitiligo was defined as “a loss of pigmentation in previously represented lesions whether repigmentation occurred spontaneously or with treatment”. The consensus statement did not specify a percentage of BSA that needed to occur for a relapse to be triggered, only that the event had to occur at least three months after treatment had ceased.
“Relapse should be assessed across multiple domains, including location of new or expanding patches, extent, involvement of facial and/or scalp hair and associated psychological distress. This multidimensional assessment reflects both clinical progression and patient-perceived effects of disease activity,” the consensus statement read.
The group was unable to agree on a consensus for social or cultural isolation and the avoidance of physical or emotional intimacy. However, these factors fall under the overall disease burden umbrella and are therefore considered as a major assessment criterion.
“The recent approval of topical Janus kinase inhibitors for the treatment of vitiligo marks a pivotal moment. However, the absence of widely accepted definitions for severity and relapse poses challenges for clinicians, health care commissioners and funding bodies internationally,” the authors concluded.
“This consensus [statement] aims to bridge the gap between physician assessment and patient experience, improve the relevance and consistency of severity classification in clinical care, research and regulatory frameworks and help close the remaining gaps in the diagnosis and classification of vitiligo.”
